Only recently has there been a renewed interest in performing both non-instrumented and instrumented spinal procedures. Analogous to outpatient shifts in total hip and knee replacement, innovation, technology and outward health care migration patterns have changed perspectives of surgeons, consumers and payors.
It is worth knowing that recent innovation and technology have expanded roles within the operating room. As a result, previous forces have shifted amongst three main stakeholders, which will continue to drive procedures from an outpatient hospital department to an ambulatory surgery center (ASC) setting.
There is a lot of emphasis on transparency and pricing of surgical cases being carried out both in hospitals, hospital-based outpatient centers and ambulatory care centers. Benefits are categorized into three groups: patient-based, surgeon-based and hospital/payor-based.
Patients are Consumers
ASCs are an attractive option for patients/consumers. Direct parking access, ease of appointments and decreased wait times, among other factors, all appeal to the hospitality and service-oriented consumer. In addition, the workflow is designed from the first time-point of registration, through pre-operative preparation, surgery and discharge. For example, a spine-based ASC would have teams that deal exclusively with spine patients, resulting in greater efficiencies and experiences. The overall duration of surgery could then be reduced due to efficient management of supplies, turnaround and radiology tech availability.
Above all, cost control remains the preeminent (financial) convenience and, as expected, the issue of cost remains pervasive amongst all stakeholders.
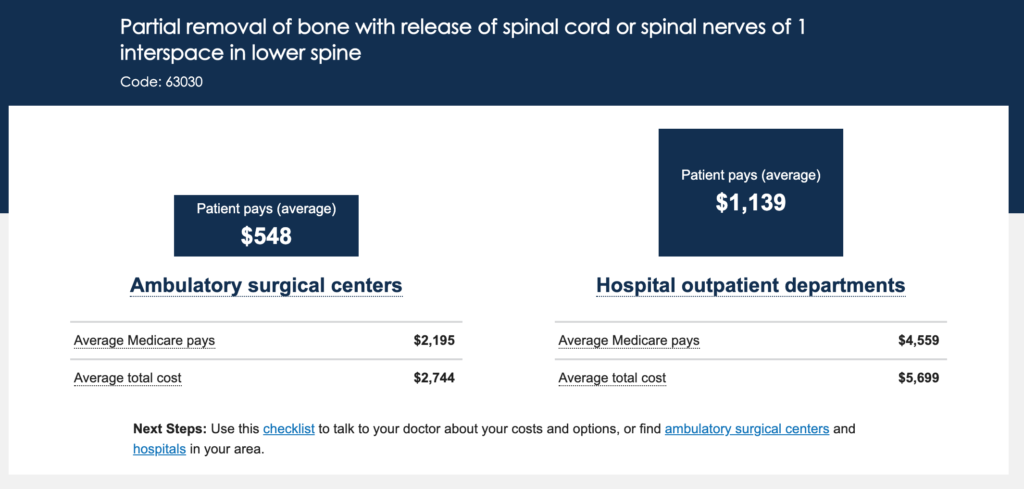
A CMS website (https://www.medicare.gov/procedure-price-lookup/) reveals not only out-of-pocket expenses for the patient, but also the total reimbursement for the hospital. The website further provides a checklist of things the patient has to ask the surgeon along with ASCs and hospitals in their area.
Below is an example of the website with CPT code 63030 (microdiscectomy), showing that the out-of-pocket expenses could be significantly higher when the procedure is performed at a hospital outpatient department (HOPD). This differential is not specific to spinal procedures. Other surgical services/procedures (i.e. cataract removal, colonoscopy, endoscopy, etc.) also have significant cost differences from the patient’s perspective.
One could then view the same scenario under a bundled payment scenario. A “bundled payment” means that the pre- and post-operative clinic fees, surgical and facility fees as well as postoperative therapies (i.e. physical therapy) are all bundled into one payment and has to be shared by all. Note that bundled payment options are already in order for joint replacement surgery. Despite the attraction, one could worry about a decrease in the number of patients receiving post-operative physical therapy or reluctance in offering surgery to patients who will require physical therapy.
Surgeons are Stakeholders
ASC operations can be financially successful for physicians. It is a straightforward disclosable issue that surgeons can have long term equity options and capture revenue from ancillary services.
Despite the financial interests, surgeons can also better position him/herself to negotiate higher rates from commercial payers and receive bonuses for surgeries done in an ASC setting from several insurance companies.
As a result, surgeons are better equipped with ASC ownership and potential leadership positions. For example, any modification or cost cutting activity would be directly related to physician-based decisions. A surgeon would no longer have to bother with compromise in quality for cost.
Payor Benefits
Cost remains as a significant issue surrounding the outward health care migration. In similar fashion, Medicare and other private insurance policy exist, stating that they have to reimburse less for surgeries performed in ASCs. Despite the reduction in payor amount, payors are slowly decreasing HOPD reimbursements, while maintaining and even incentivizing ASC reimbursements. Patient co-pays (as mentioned above) have been seen to be lower for procedures in the ASC setting. Therefore, all payor behavior remains supportive. As a result, health care hospital chains and universities are acquiring ambulatory care centers at an increasing rate.
Challenges and Opportunities Remain in the ASC Setting
Case volume, OR turnover time, patient selection, surgical skill, risk assessment and risk avoidance are just few topics that need development and standardization. Likewise, financial and other operational challenges may remain. For example, some ASCs may operate on a very low margin and therefore require many efficient systems to remain positive. Some may estimate nearly 150% case load growth in order to maintain the business.
Despite the necessity, there remains an opportunity. Ambulatory spine surgery will benefit from continued alignment of the above stakeholders’ interests. Also, in the near future, CMS procedure acceptance could expand.

Karthik Madhavan, MD
University of Miami

Scott J. Raffa, MD
Memorial Healthcare System