

Lora K. Fogam, MD
Windsor University School of Medicine
and
Laura B. Ngwenya, MD, PhD, FAANS
University of Cincinnati
Traumatic Brain Injury (TBI) is a major global health problem, causing greater than 5,800,000 deaths annually and widespread disability(1) . The economic cost of TBIs to the United States currently stands at 4.2 Trillion, 327 Billion in medical insurance and a related work loss cost of about 69 Billion. However, according to data from the Committee on Advanced Specialty Training (CAST), acquired in March 2023, only 2.5% of the approximately 160 graduating neurosurgery residents per year, chose to pursue a Neurotrauma Fellowship. This is in contrast to the 16.4% that chose a Spine Fellowship, 16.4% Pediatrics Fellowship and 9.5% Cerebrovascular Fellowship. With only 2.5% of 160 (~4) graduating neurosurgery residents receiving specialized training in neurotrauma, there is concern that there is a mismatch between the number of Level I Trauma Centers, and the number of self-identified neurotrauma neurosurgeons.
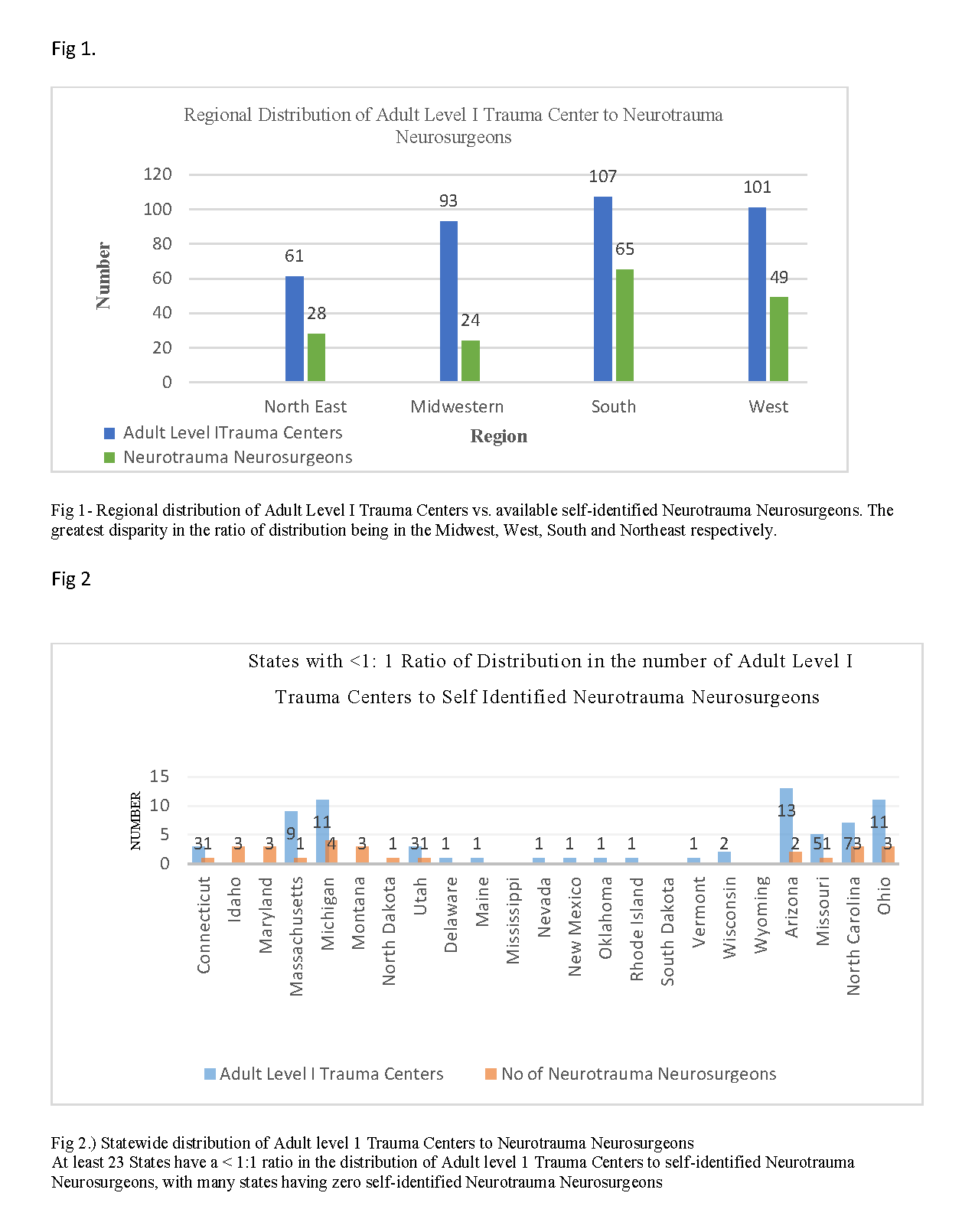
Data from the Center for Disease Control (CDC; TBI Surveillance Reports 2014, 2016, 2017, 2018, 2019, 2020), the American Association of Neurological Surgeons (AANS)(13), and published manuscripts suggests that there are currently 23 states with fewer neurotrauma-dedicated neurosurgeons than there are Level 1 Trauma centers in the state, a less than 1:1 ratio (6).
Currently, there are 166 self- identified neurotrauma surgeons as per AANS membership(13). This is in the context of approximately 4,897,139 TBI operative cases (1, 2), a steady increase in the US population at a rate of 7.10% between 2010-2020 per the US Census Bureau (15) and CDC data indicates a 13% rise in TBIs between 2014 -2021 (4, 5). Published data from the American Medical Association (AMA) suggests a projected shortage of 1,200 neurosurgeons by 2025. The low number of neurotrauma neurosurgeons, with the already identified projected neurosurgeon shortage, creates a potential disparity in the ability to provide neurotrauma expertise in areas of need.
We identified states within regions of the United states with a significant disparity, as those that have a huge disproportion between the number of Adult ACS Certified Level I Trauma Centers and the number of neurotrauma neurosurgeons available. (Figure 1), at the time of data collection, the Midwest had the largest gap between the number of Adult Level I Trauma Centers and number of self-identified neurotrauma neurosurgeons. Ohio has 11 Adult Level I Trauma Centers and only three self-identified neurotrauma neurosurgeons, Michigan has 11 Adult Level I Trauma Centers and four self-identified neurotrauma neurosurgeons. South Dakota has neither an Adult Level I Trauma Center nor a self-identified neurotrauma neurosurgeon. Missouri has five Adult Level I Trauma Centers and only one self-identified neurotrauma neurosurgeon. Within the Western Region, Arizona has 13 Adult Level I Trauma Centers and two self-identified neurotrauma neurosurgeons. In the North East Region, Massachusetts has nine Adult Level 1 Trauma Centers and one self-identifying neurotrauma neurosurgeon. Finally, within the Southern region North Carolina has seven Adult level I Centers and three self-identifying neurotrauma neurosurgeons, while Mississippi lacked ACS Level I trauma centers and self-identified neurotrauma neurosurgeons.(6)
While access to a trauma center is one barrier, having enough dedicated neurotrauma neurosurgeons to staff these hospitals is a separate, but related problem. While any neurosurgeons can take trauma call, trauma centers with self-identified and dedicated neurotrauma neurosurgeons are more likely to take more advanced measures in patient care, which is often necessary at Level I Trauma Centers. Additionally, it has been shown that consistently following guidelines and having a dedicated neurotrauma team can positively impact patient outcomes (3)
Of the CAST-approved fellowships in the United States, data at the time of this printing show only six neurotrauma fellowships. In contrast, there are: 69 CNS endovascular fellowship programs, 51 spine fellowship programs, 38 stereotactic and functional neurosurgery fellowship programs, 30 neurocritical care fellowship programs, 26 neurosurgical – oncology fellowship programs, 18 skull base fellowship programs, 11 cerebrovascular fellowship programs and 10 peripheral nerve fellowship programs. With approximately four graduates a year choosing a neurotrauma fellowship, in order to staff every Adult Level I Trauma Center with a self-identified neurotrauma neurosurgeon, a total of 76 more self-identified neurotrauma neurosurgeons would be required to offset the current disparity. Maintaining the current recruitment into neurotrauma fellowships would take ~19 years to fill the gap, without accounting for any growth in numbers of trauma centers. Hence measures should be considered to garner interest and retention into the subspecialty of Neurotrauma.
References:
1 ) Neurotrauma Surveillance in National Registries of Low-and Middle-Income Countries: A Scoping Review and Comparative Analysis of Data Dictionaries
Ernest J Barthélemy , Anna E C Hackenberg Jacob Lepard , Joanna Ashby , Rebecca B Baron , Ella Cohen , Jacquelyn Corley , Kee B Park
- Emergency department visits for head trauma in the United States Christopher E. Gaw1 and Mark R. Zonfrill
- Establishing a Traumatic Brain Injury Program of Care: Bench marking Outcomes after Institutional Adoption of Evidence- Based Guidelines Phiroz E .Tarapore, Mary J. Vassar, Shelly Cooper, Twyila Lay, Julia Galletly,Geoffrey T . Manley, Michael C Huang
- CDC Surveillance Report of Traumatic Brain Injury-related Emergency Department Visits, Hospitalizations, and Deaths United Sates, 2014
- CDC TBI Surveillance report United States 2018 and 2019
- List of trauma centers in the United States Verified by American College of Surgeons
7 ) Differences in State Traumatic Brain Injury–Related Deaths, by Principal Mechanism of Injury, Intent, and Percentage of Population Living in Rural Areas — United States, 2016–2018 Jill Daugherty, PhD1; Hong Zhou, MS, MPH1; Kelly Sarmiento, MPH1; Dana Waltzman, PhD
8 ) Traumatic Brain Injury–Related Deaths by Race/Ethnicity, Sex, Intent, and Mechanism of Injury — United States, 2000–2017 Jill Daugherty, PhD1; Dana Waltzman, PhD1; Kelly Sarmiento, MPH1; Likang Xu, MD
9 ) The Epidemiology of Emergency Department Trauma Discharges in the United States Charles J. DiMaggio, PhD, MPHa,c,* , Jacob B. Avraham, MDa, David C. Lee, MDb,c , Spiros G. Frangos, MD, MPHa, and Stephen P. Wall, MD
10 ) Neurosurgical Coverage Essential, Desired, or Irrelevant for Good Patient Care and Trauma Center Status Thomas J. Esposito, MD, MPH, R. Lawrence Reed II, MD, Richard L. Gamelli, MD, and Fred A. Luchette, MD
11 ) State-Level Numbers and Rates of Traumatic Brain InjuryRelated Emergency Department Visits, Hospitalizations, and Deaths in 2014 Jill Daugherty, PhD, MPH, Karen Thomas, MPH, Dana Waltzman, PhD, Kelly Sarmiento, MPH
12 ) Academic Neurosurgical Fellowship training programs, Society of Neurological Surgeons ,Accredited Neurosurgery programs ,Accreditation Council for Graduate Medical Education (ACGME),
13 ) American Association of Neurological Surgeons AANS/ Congress of Neurological Surgeons (CNS)
14 ) Committee on advanced sub-specialty Training (CAST)
15 ) United States Census Bureau